
Earlier this week, Spectrum News (SFARI as was) carried an interesting and disturbing story about a $2,000 test purporting to identify babies at risk of autism based on an analysis of their placenta.
The test has been trademarked as PlacentASD by Dr Harvey Kliman of the Yale School of Medicine and promoted on the Yale website. In a slick marketing video, Kliman describes the rationale for the test:
The big issue in autism has been diagnosing autism earlier… The earlier you can diagnose the chance of having autism the better the outcome. The problem has been how do we do that and really up til now there hasn’t been a way to that. But based on research we’ve been doing here in my laboratory at the Yale School of Medicine we figured out a way to diagnose autism risk at birth.
What we’re looking for are the abnormal trophoblast inclusions or abnormal folds of the sections of the placenta. What I do is count how many I see and in the four slides if I see three or more of these trophoblast inclusions we know that that placenta comes from a child who is at increased risk for developing autism. It doesn’t mean that they will develop autism it simply means that they’re at increased risk for developing autism.
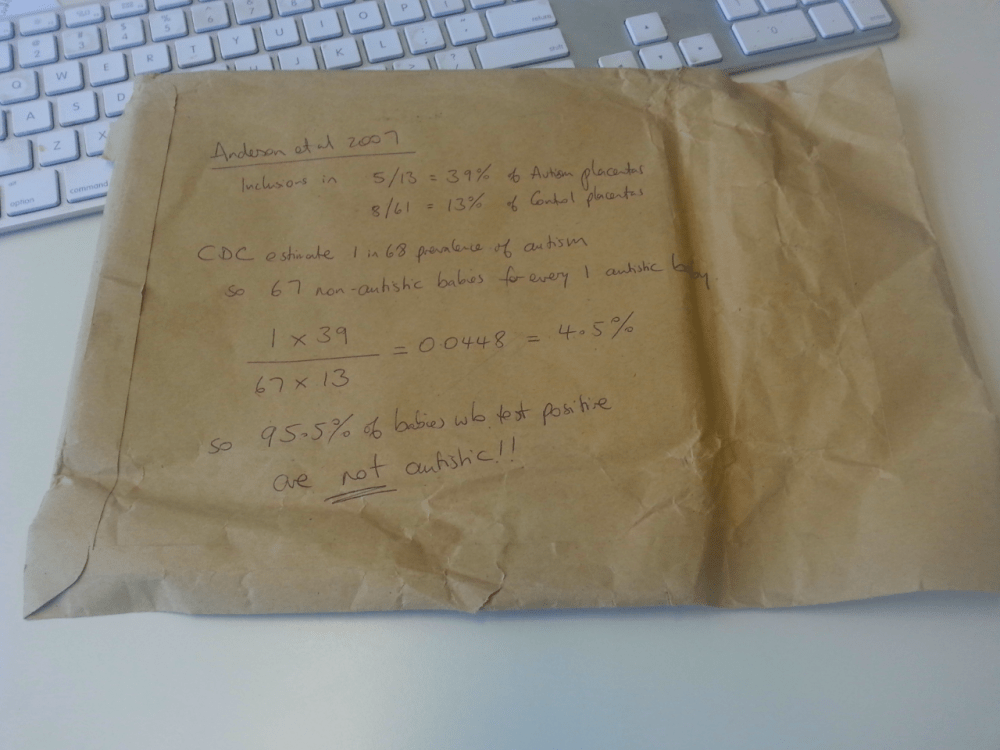
The PlacentASD test is based on a 2007 study by Kliman and colleagues at Yale, which found increased rates of trophoblast inclusions (small folds) in the placentas of babies who were later diagnosed with autism.
The study was small with only 13 placentas in the autism group and the effect reported was barely statistically significant (p = .044). The authors at the time were appropriately cautious, concluding:
Although probably not functionally detrimental or causative, the greater occurrence of placental trophoblast inclusions observed in ASD individuals may reflect altered early developmental processes. Further research is required to replicate the basic finding, to understand the basis for the trophoblastic abnormality, and to determine the utility of the measure in early detection of ASD.
So has there been any further research to justify the marketing of a $2,000 test? A cited reference search on Google Scholar indicates that there have been no published replications in the 9 years since that original study. The closest is a 2013 study looking at the placentas of babies with an older sibling with autism – but this didn’t differentiate between babies who did or did not subsequently get an autism diagnosis.
Even if there is a reliable link between placental abnormalities and autism, the 2007 study already suggests that the test is not particularly accurate. Only 5 of the 13 “autism placentas” (39%) had inclusions, so the test completely missed the majority of babies who went on to get an autism diagnosis.
Even more worryingly, 8 of the 61 placentas in the control group also had inclusions. A 13% false positive rate might not sound too bad. But this neglects the base rate – the fact that most babies in the general population are not autistic. As a result, we can expect the vast majority of positive PlacentASD results to be false positives. This is because 13% of a large number of non-autistic babies is a lot more than 39% of a very small number of actually autistic babies.
According to my back-of-the-envelope calculations, based on the latest figures for autism prevalence in the general population, less than 5% of the babies who tested positive would actually go on to an autism diagnosis.
The concern, of course, is that parents getting a positive test result won’t realise how uninformative the $2,000 test really is. They won’t be counselled that, despite the positive result, their child is still highly unlikely to be autistic. And they will find themselves filtering every quirky behaviour of their child through the lense of “autism risk”.
The PlacentASD video includes an interview with Chris Mann Sullivan, whose daughter’s test returned positive. She illustrates this point beautifully:
So here’s an example of something I don’t think I would have caught had I not been aware that she had a positive PlacentASD test. I would not have caught the fact that she was not responding to loud noises sounds and eventually her name when you were standing at a certain distance behind her.
Worth noting is that George Anderson, first author of the 2007 study, has distanced himself from his colleague’s rush to market. In a blistering commentary, entitled Two Proposed Early Biomarker Tests of ASD: More Harm Than Good, he criticises the “placenta test” and a second biomarker based on maternal antibodies, raising precisely these issues:
The marketing and clinical application of the MAR and placenta tests as they stand would have serious detrimental effects. Typically developing children misidentified as being at risk might be subjected to unnecessary, intrusive and expensive interventions. Such misidentified children would suffer from labeling effects and altered intra-family dynamics, and their families would experience needless anxiety and stress. Conversely, a large proportion of the families of children who go on to develop autism would be falsely reassured that their child was not at risk.
It’s also worth noting that these concerns aren’t specific to these two tests. Similar problems affect proposed genetic, eye-tracking, and voice analysis markers of autism. Even with tests that do reliably differentiate between autistic and non-autistic infants, performance in the real world is not great.
There’s currently a heated debate about introducing autism screening for all infants in the United States. The key question is whether the benefits of perhaps identifying some kids earlier outweigh the costs of screening and the inevitable false positives that will ensue, the needless financial and emotional stress it might place on families, and the resources it might take away from kids who really needed them. PlacentASD is an egregious example, but it serves as a good illustration of the issues that researchers, advocates, and policy makers should all be considering.
Reference
Anderson GM, & Stahl SS (2014). Two proposed early biomarker tests of ASD: more harm than good. Journal of autism and developmental disorders, 44 (4), 988-9 PMID: 24174282

2 thoughts on “Autism biomarkers – not ready for market”